
What a tangled web we may have weaved & What is Really Ailing You?
What a tangled web we may have weaved & What is Really Ailing You?
+ Why Remdesvir was a death trap
What’s Really Ailing Us?
below…
A few words on spider butts, (self-assembling) hydrogels and proteinaceous obstructions discovered in autopsies

Nov 5, 2023
A paper was published back in August 2022 entitled: “Spidroin N-terminal domain forms amyloid-like fibril based hydrogels and provides a protein immobilization platform”.1 It was published by a group out of Sweden and involves an investigation into the usefulness of spider silk proteins as scaffolding for biotech purposes.

The reason I am bringing this paper up now (and summarizing it) is because it was recently linked to our preprint about DNA contamination in the COVID modified mRNA products by a follower on Twitter. The reason it was linked was because of the mystery open reading frame (ORF) discovered in the plasmids snapgened by Kevin McKernan, and also discussed in the publication entitled: “Are There Hidden Genes in DNA/RNA Vaccines?”.2
ORFs are spans of DNA between start and stop codons. Start and stop codons are the triplets of bases (in messenger RNA) that command the commencement and ending of translation in a protein. Whatever that protein may be.
So what’s the problem, you ask? Well, it’s not just that this ORF is absolutely not meant to be in the plasmid, just like the DNA is not meant to be in the vials. It’s not just that this ORF was absolutely not disclosed by Pfizer in their plasmid map, just like the SV40 elements were not disclosed.
WHO and FDA guidelines exist to prevent biological whoopsies like inclusion of superfluous potentially ‘active’ ORFs that may end up in in vivo contexts. The following paragraph is an excerpt taken verbatim from the WHO Technical Report Series No 941, 2007 Guidelines for assuring the quality and nonclinical safety evaluation of DNA vaccines.
…a DNA sequence homology check of the plasmid with the international databases (e.g. the National Center for Biotechnology Information, National Institute for Health, USA, and/or other international nucleotide databases) should be performed to investigate the presence of unintended sequences of biological significance such as those encoding cellular growth functions or alternative and unanticipated reading frames.3
These guidelines exist for very good reasons that go far beyond optimizing plasmids for use in vaccine component production: they exist because we really want to prevent mystery ORFs in biological product settings because of the risk of translatable ‘undesirable’ proteins (ahem - like amyloids) that may have unintended clinical outcomes in the in vivo setting (aka: adverse events). This particular ORF that Kevin found is exceedingly odd in that it is the antisense of the spike itself, although it has no known function as a protein.
The punchline is that when Kevin BLASTed this ORF in UniProt, he found that it has weak sequence homology (25.3%) to Major ampullate spidroin 1 MaSp1. The source organism listed is a bacterium called Nitrospirillum amazonense Y2. This MaSp1 is one of 2 types (the other one is MaSp2) used to make a specialized type of spider silk which is also the crux element of the paper.
Two open questions on our minds: Are superfluous whoopsie proteins being made in some people who were injected with the modified mRNA COVID-19 products? Do the vials contain DNA contaminant-associated amyloid-encoding genetic material?
I’ve already written extensively on the amyloidogenic nature of the spike protein but maybe this is yet another way for the circulatory system to get ‘gummed up’?
On spidroins
Spidroins are not an 80s band from Toronto but, in fact, spidroins are proteins used to make spider silk.
Interesting tidbit: You can’t farm spider silk like you can silkworm silk because spiders tend to eat each other. Not very profitable as a business. Better to use Crispr-Cas to gene edit silkworms to make them make spider silk?4
Spidroins are part of a large group of proteins called scleroproteins that also includes other structural proteins like keratin and collagen.5 The major ampullate spidroins (MaSp1 and 2 - mainly consisting of highly repetitive glycine and alanine blocks6) so-called because they are secreted by the major ampullate gland in spiders, are thus used for creating Dragline silk for those spider thrill seekers who rapel across Europe, and spin webs, and fly, and… transferance of sex hormones?

Silk produced by females provides a transmission channel for male vibratory courtship signals, while webs and draglines provide a substrate for female sex pheromones.7
Amazingly, the role of male-produced silk in mating is ‘under-studied’.8
Spidroin is really important composition-wise in dragline silk because of its associated toughness and strength. However, there many different types of spider silk composed of different types of proteins, including spidroins, all with specific functions. Shown in Figure 3 on the left are the various types of silks used for web construction with a little black spider hanging from a Dragline. Each of these silks has their own protein compositions, including spidroin proteins, and originate from different glands of which some spiders, like Araneus diadematus, have 7. On the right is a proposed model for Dragline composition and structure involving various protein structures (including secondary structures: beta sheets and alpha helices) interconnected by an amorphous matrix.
![Schematic of the spider's orb web, structural modules, and spider silk structure.[15] On the left is shown a schematic drawing of an orb web. The red lines represent the dragline, radial line, and frame lines, the blue lines represent the spiral line, and the centre of the orb web is called the "hub". Sticky balls drawn in blue are made at equal intervals on the spiral line with viscous material secreted from the aggregate gland. Attachment cement secreted from the piriform gland is used to connect and fix different lines. Microscopically, the spider silk secondary structure is formed of spidroin and is said to have the structure shown on the right side. In the dragline and radial line, a crystalline β-sheet and an amorphous helical structure are interwoven. The large amount of β-spiral structure gives elastic properties to the capture part of the orb web. In the structural modules diagram, a microscopic structure of dragline and radial lines is shown, composed mainly of two proteins of MaSp1 and MaSp2, as shown in the upper central part. In the spiral line, there is no crystalline β-sheet region.](https://substackcdn.com/image/fetch/f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fca7a3c0e-6632-4f39-8173-f109c9185a7c_900x381.png "Schematic of the spider's orb web, structural modules, and spider silk structure.[15] On the left is shown a schematic drawing of an orb web. The red lines represent the dragline, radial line, and frame lines, the blue lines represent the spiral line, and the centre of the orb web is called the \"hub\". Sticky balls drawn in blue are made at equal intervals on the spiral line with viscous material secreted from the aggregate gland. Attachment cement secreted from the piriform gland is used to connect and fix different lines. Microscopically, the spider silk secondary structure is formed of spidroin and is said to have the structure shown on the right side. In the dragline and radial line, a crystalline β-sheet and an amorphous helical structure are interwoven. The large amount of β-spiral structure gives elastic properties to the capture part of the orb web. In the structural modules diagram, a microscopic structure of dragline and radial lines is shown, composed mainly of two proteins of MaSp1 and MaSp2, as shown in the upper central part. In the spiral line, there is no crystalline β-sheet region.")
Inside the spider’s hindquarters (aka: spider butt), is the major ampullate gland as shown below in Figure 4. The Dragline silk is produced from spidroins that are stored in the major ampullate gland. It is a pipeline of decreasing diameter with chamber-associated specific physiological, physical and chemical characteristics, that allows for almost instant production of super strong/tough silk fibers by pulling, from the stored spidroin proteins.
")
The pulling/spinning is done by the spinnerets on the ass-end of the spider.

Dragline silk has incredibly high tensile strength and ductility (flexible) making it perfect as the spider’s bungy-jumping lifeline. This is why humans are so interested in copying it for repurposing as biomaterials. In fact, it is actually tougher than both kevlar and steel. It’s absolutely mind-blowing to me that Draglines also have torsional memory. This is why the spider doesn’t spin or twist when ‘hanging by a thread’.9
Not only are medical and biotech arenas trying to get in on the spider silk action, but the military are as well. For example, spider silk technology is used in the production of bullet-proof vests. You might also find it interesting that as far back as 2011, there have been published works on introducing recombinant silk proteins into mammals for ‘regenerative medicine’.1011
Furthermore, fibers developed from spidroin are tolerated in vitro, in cell culture, and in vivo, in animals like pigs, as no signs of either inflammatory response nor body reaction were shown to these fibers. These results suggest that they could be used in medicine without risk of biocompatibility issues and thus potentially lead to many new opportunities in tissue engineering and regenerative medicine.12
On N-terminal (NT) domains
N-terminal domains are one of the two bookends of each amino acid (remember there are 21 amino acids in eukaryotes) and effectively also bookend proteins or protein chains (polypeptides). They are called N-terminal because they involve the presence of a Nitrogen (N) atom in the form of an NH2. The other bookend is called the Carboxyl-terminus or C-terminal because they involve the presence of a Carbon (C) atom in the form of a COOH. Let’s refer to the N-terminus as the head and the C-terminus as the tail. Each amino acid is bonded (a covalent chemical bond called a peptide bond) from head to tail and thus, all protein chains and all proteins in general, will have an N and a C-terminal. If you think of an amino acid as a pearl, then a ‘string’ of pearls would be akin to primary protein structure whereby the string linking the pearls would be the peptide bonds formed between the amino acids via the N and C-terminals. When these strings are bonded by hydrogen bonds side-by-each, they are called beta sheets, and when they are coiled they are called alpha helices. These are the secondary protein structures that we all know and love.

For more introductory and specific context from the paper, the NT domains in the paper are alpha helical as depicted in Figure 7 (pdb - 4fbs).

On hydrogels
Hydrogels are 3-dimensional cross-linked fibrous structures held together either by chemical (covalent) or physical (hydrogen) bonds, electrostatic interactions, van der Waals forces, or physical entanglements.13
…Or if you like the Wikipedia definition:
A hydrogel is a biphasic material, a mixture of porous, permeable solids and at least 10% by weight or volume of interstitial fluid composed completely or mainly by water. In hydrogels the porous permeable solid is a water insoluble three dimensional network of natural or synthetic polymers and a fluid, having absorbed a large amount of water or biological fluids.14
Figure 8 shows a schematic demonstrating the formation of the cross-linking of self-assembled nanofibers. Basically, hydrogels are 3-D meshes of hydrophillic nanofibers bound together.

Hydrogels are used to make such glorious things as contact lenses15, biosensors and glues. They are inspired by natural hydrogels such as gelatin (derived from collagen). There is nothing so new about hydrogels in biotech and industry, and they have been being developed and used for decades, but applications and variations continue to expand.
Hydrogels are classified based on many factors such as the composition of the nanofibers (polymers) used, the way they are cross-linked, how they respond to stimuli, as shown in Figure 9, and their ionic charge.

I highly recommend reading the papers entitled: “Fundamental Concepts of Hydrogels: Synthesis, Properties, and Their Applications”16 and “Hydrogels: Properties and Applications in Biomedicine”17 for comprehensive information pertaining to hydrogels.
In the abstract of the spidroin paper, the authors write:
Here, we report that recombinant miniature spidroins, and importantly also the N-terminal domain (NT) on its own, rapidly form self-supporting and transparent hydrogels at 37 °C.
…we find that NT and miniature spidroins undergo a structural transition into β-sheets and amyloid-like fibrils upon gel formation.
Figure 10 (Figure 8 from the paper) shows an overview of NT gelation. Gelation is the act of going into gel form. Interestingly, the NT samples incubated at pH 8 and 7 both gelled after 30 min at 37 °C but they differed by clarity: the pH 8 gel remained clear and the pH 7 gel was more opaque (shown in Figure 11). Figure 10 shows the NT alone and NT tagged with green fluorescent protein (GFP) and purine nucleoside phosphorylase (PNP). The main reason the authors got excited was that they were able to fuse other proteins to the recombinant only-NT domain and form hydrogels with the embedded proteins remaining functional. And again, these hydrogels comprise amyloid-like fibrils.

Some of the mysteries being unraveled in spider silk science include how spiders maintain spidroin solubity in the ampulla and also how they produce/spin the silk so fast ‘out of storage’. It turns out it has a lot to do with the changing physiological conditions in the glands of the spider that alter the stability and structures of the N and C-terminal domains of the spidroins.18
Part of the biotech of spidroin science involves looking at the effects of changing various physiological parameters like pH, and determining how this affects fiber production and quality. What the authors found from their studies was that when they incubated recombinant mini-spidroins at 37°C, they were able to form hydrogels whereby a structural transition from α-helix into β-sheets resulted in the formation of amyloid-like fibrils.
The finding that NT on its own could form gels was unexpected considering the common notion that NT is a highly soluble and stable protein and that previous reports of recombinant spidroin hydrogels have attributed the gelation effect to conformational changes in the repetitive region and/or CT.
I would like refer to a paper entitled: “Decoding the secrets of spider silk” by Eisoldt et al.19 to show a cartoon version of the journey of the spidroin proteins to assembled fibers from tail to exterior via the major ampulate gland. I think it is important to understand what the spidroins go through to end up as stable NT-dimerized β-sheet-rich proteins that enable fiber assembly. This is more for me to mentally compare the spider stuff with what they did in the paper.
You can see from this neat schematic that the spidroins start off as secreted proteins and get stored at very high concentrations (50%) in the ampulla with liquid crystalline properties. Spidroins form micellar-like structures controlled by their amphiphilicity to prevent irreversible aggregation. The micellar-structures undergo chemically and physically-induced changes in the duct and move through sequentially smaller diameter spaces with sequentially lower pHs to ultimately result in assembled fibers by removal of water, dimerization of the NT domains, beta sheet formation and protein alignment.20 This is shown in the bottom right corner.

On the subject matter of the spider stuff, the authors of the spidroin paper write:
NT is monomeric under conditions that reflect those in the gland lumen and mediates solubility to the spidroins, but at decreased pH, protonation of a series of carboxylate side chains leads to NT dimerization with a pKa of around 6.5, which stabilizes NT and locks the spidroins in large networks. Thus, NT plays a key role in the silk formation process by transitioning from a monomer in the dope to a dimer in the fiber.
The important difference between the spider stuff21 and the recombinant lab stuff is the way in which the fibers form and it is kind of surprising, ie: α-helix dimerization and β-sheet formation/protein alignment in the former, and α-helix conversion into β-sheets in the latter using temperature as a means to induce gel formation.
Even though I feel I don’t quite yet understand the spider or the recombinant lab stuff, it is an amazing thing that people are doing with regard to the latter: making recombinant spidroins that form hydrogels. It is even more amazing that these synthetics can self-assemble into a variety of shapes, films or hydrogels.
I do highly recommend reading the decoding paper. It’s so awesome. They write:
So far, no biomimetic spinning process exists that would allow the formation of native-like spider silk fibers from recombinant silk proteins. However, despite the nonexistent spinning process most recombinant spider silks can self-assemble into non-natural shapes such as spheres, capsules, films, non-wovens or hydrogels (Fig. 5), which have a high application potential.

So what have we learned?
The spidroin paper is all about rapid formation of self-supporting and transparent hydrogels from recombinant spidroins - and NT on its own - in meh conditions. ‘The gelation is caused by NT α-helix to β-sheet conversion and formation of amyloid-like fibrils.’
So where does that leave us with our original question?
Are superfluous whoopsie proteins being made in some people who were injected with the modified mRNA COVID-19 products?
It might be the case. We need to find out.
Do the vials contain DNA contaminant-associated amyloid-encoding genetic material?
They might. We need to find out if any proteins and what proteins, are being passed to people and if these proteins are being translated. And if they are being translated, what are they being translated into?
Could it be that amyloidogenic peptides akin to spidroin are being translated in people and subsequently creating immobilizing hydrogel scaffolds for other proteins?
Comments welcome → here
Remdesivir
On Gilead Sciences and “A Remedy Worse than the Malady”


Conversely, the hospitals did receive a massive financial incentive to diagnose patients with COVID-19, administer remdesivir rather ivermectin or hydroxychloroquine and to place patients on ventilators. Here, I do believe the payoff was large enough to argue it influenced medical decision making. - AMD
Dr. Paul Marik is the 2nd most published critical care doctor in the history of medicine with more than 500 peer reviewed papers and books with over 43,000 citations of his work and a scholarly “H” rating, higher than many Nobel Prize winners. - @darkymax
Late last year, in December 2022, my mother went into hospital.
The frail 75-year-old, after 3 years of the pandemic we had to have, finally managed to “catch covid” in hospital. Well, she had a mild sniffle, so two nurses wearing hazmat suits came in to Rapid Antigen Test her. It came up positive. Mum told me that they turned to each other, with fear in their eyes, as if they were in the midst of the grim reaper himself.
Mum was sharing the room with a lady who was half deaf, and who’s TV was damaging her ear drums all day. So, she was quite relieved when they quickly escorted the lady out of the room, to save her from the dreaded virus, and give mum a full week of peace and quiet while in “isolation”.
When I spoke to her on the phone, she said that the nurses and doctors were telling her to not worry, as they had antivirals for her. I told her to tell them that they were not allowed to give her anything without my approval and to get the doctor to call me.
And so, he did, the next day.
From his accent I knew he was from Iran, probably immigrated to Australia relatively recently. He didn’t sound annoyed at having to call me.
He said that they wanted to give mum some antivirals to help her with her covid, but that she had told him to call me.
“I assume it’s either Remdesivir or Paxlovid, you want to give her?” I asked.
“Yes, that’s right, you know about them?” He said, with a hint of pleasant surprise that he might be talking to an understanding peer.
“Yes, I do. I want to be very clear. Under no circumstance whatsoever are you allowed to give her either of those two drugs. In fact, you are not allowed to give her anything without my prior approval. You are only allowed to give her some supplements such as Vit C, D and Zinc. Can you please confirm that we have an understanding?”
I was now expecting some resistance, some indignation, at the very least some attitude. I didn’t get any.
“Yes, I understand. That won’t be a problem.”
This is December 2022. I am sure that if I had tried that moved in December 2020, or even 2021, I would have had the bruised ego of the medical class to contend with. But he rolled over like a puppy.
So, I pressed on.
“I don’t know about you, but neither I, nor more importantly my mother, are afraid of covid. As far as we are concerned, we are happy to treat it the way we would a common cold.”
And here is the punchline, delivered by mum’s surrendered, and frankly quite pleasant, Iranian Australian doctor.
“Look, I’ve had four doses of the vaccine and had covid twice, so I don’t know what to think anymore.”
And with that we farewelled each other.
I genuinely hate hospitals now. Home to these dangerous knuckleheads and their poisons.
Anyway, I smuggled in some ivermectin to her the next day, just to be on the safe side, and two days later she was fine.
I’ve mentioned Remdesivir several times over the last couple of years of writing, but I wanted to write a standalone piece on it, aimed at the recently awakening. It’s never too late to wake up and exit the Truman Show, and if so inclined, do a bit of homework on stuff you might have missed.
Going into Bobby’s masterpiece, The Real Anthony Fauci (TRAF), I knew enough about Remdesivir to know if was evil and to be avoided. But I didn’t know it was a failed Ebola drug.
Yes, that’s right. They pulled it from the trials as it was deemed too dangerous, even against Ebola.
Much of the “death by hospital” can be put down to Remdesivir.
If you know anyone that died in hospital “from covid”, check to see how much Remdesivir they gave them.
In Oct 2022 I wrote this:
Fraud By Omission - Lies are Unbekoming (substack.com)
Australia loves Remdesivir, it was approved early, in July 2020.
But if you go into the Product Information you will find this on page 6. pdf (tga.gov.au)
Renal impairment
In animal studies on rats and monkeys, severe renal toxicity was observed (see section 5.3). The mechanism of this renal toxicity is not fully understood. A relevance for humans cannot be excluded.
This from Nov 2020 is the best essay on the subject.
Remdesivir, Hydroxychloroquine and COVID-19 – Quadrant Online
Investigative reporter Sharyl Attkisson reported in a story on the US program Full Measure on May 18 that eleven members of the NIH’s COVID-19 Treatment Guidelines Panel reported links to a drug company, nine of them declaring relationships to Gilead. Seven more, including two of the committee’s leaders, had ties to Gilead beyond the eleven months they were required to disclose. Two were on Gilead’s advisory board, while others were either paid consultants or had received research support and honoraria. The endorsement of remdesivir and veering away from HCQ was perhaps, therefore, not surprising. (A perhaps even more alarming conflict of interest emerged in the United Kingdom, where it was revealed that the Chief Scientific Officer, Sir Patrick Vallance had £600,000 worth of shares in the vaccine maker contracted by the government to make the UK’s coronavirus vaccine.)
Gilead Sciences has played a very sinister part in the covid show, but it remains a name that is in most people’s blind spot.
Next there is this from the 2017 SPARS pandemic prep simulations.
War Games - Lies are Unbekoming (substack.com)
According to the scenario narrative, a so-called “SPARS” coronavirus ignites in the United States in January 2025 (the COVID-19 pandemic began in January 2020). As the WHO declares a global emergency, the federal government contracts a fictional firm that resembles Moderna. Consistent with Gates’s seeming preference for diabolical cognomens, the firm is dubbed “CynBio” (Sin-Bio) to develop an innovative vaccine using new “plug-and-play” technology. In the scenario, and now in real life, Federal health officials invoke the PREP Act to provide vaccine makers liability protection.
Another company in this scenario receives an Emergency Use Authorization for a remdesivir-like antiviral named Kalocivir that federal officials previously evaluated as a therapeutic for SARS and MERS.
This item seems to predict Dr. Fauci and Bill Gates’s aggressive promotion of a failed Ebola drug, remdesivir, during the pandemic as “Standard of Care” for COVID-19. Dr. Fauci helped develop the drug, and Gates has a substantial equity stake in its manufacturer, Gilead. The two men promoted remdesivir during the earlier Ebola and Zika pandemics, despite its stunning inadequacy as a remedy for these ailments. Promotion of remdesivir, and the simultaneous Gates/Fauci orchestrated suppression of ivermectin and hydroxychloroquine, collectively—as we shall see— caused hundreds of thousands of deaths in the United States alone.
Interesting that the hypothetical anti-viral, as far back as 2017 was also an “-ivir”.
They sure like telling us beforehand and rubbing our nose in it.
As most of you know by now, I think, covid was AIDS 2.0. Much bigger and better, with far more reach and scale. Remdesivir played its part.
AIDS v2.0 - Lies are Unbekoming (substack.com)
What we are experiencing today is HIV/AIDS version 2.0, but that will not make sense without reading Kennedy’s book.
The narrative in version 1.0, that built the first mega industry, was that there was a deadly virus (HIV) that caused a deadly disease (AIDS) that was tested for with a special test (PCR) that required a specific new solution (AZT) while preventing existing cheap and effective treatments (Bactrim) and silencing critics (Duesberg).
Today’s narrative version 2.0, that has built this new mega industry says, there is a deadly virus (Sars-Cov-2) that causes a deadly disease (Covid19) that is detected by a special test (PCR) and has a specific new solution (Remdesivir and genetic “vaccines”) while preventing existing cheap treatments (Ivermectin) and silencing critics (Yeadon, McCullough, Malone etc.).
Sound familiar?
With that, I want to leave you with Bobby’s explanation from TRAF of Remdesivir.
TRAF, for me, remains the best high level telling of the Remdesivir story, for someone brand new to the subject.
This is a very important part of the history of what I call the Global Medical Crisis (GMC) and one that perfectly encapsulates the sociopathy and depravity of the people that opened these doors of hell.
With final and eternal thanks to Robert Kennedy Jr. I hope he forgives me my copyright sins. I have done my best to get as many people as possible to buy the book.
It’s never too late to buy and share the book. It remains the best book on the GMC. Just look at the reviews.
Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health
Remdesevir and Fauci
Anthony Fauci needed to use all his moxie and all his esoteric bureaucratic manoeuvres—mastered during his half-century at NIH—to win FDA’s approval for his vanity drug, remdesivir. Remdesivir has no clinical efficacy against COVID, according to every legitimate study. Worse, it is deadly poisonous, and expensive poison at $3,000 for treatment. In fact, remdesivir’s wholesale cost is roughly 1,000x more costly than hydroxychloroquine and ivermectin. The challenge required Dr. Fauci to first sabotage HCQ and IVM. Under federal rules discussed earlier, FDA’s recognition of HCQ and IVM efficacy would automatically kill remdesivir’s ambitions for EUA designation. And even if Dr. Fauci somehow finagled an FDA license for remdesivir, demand for the product, which doctors were administering late in the disease, as it had to be given through an IV in the hospital, would plummet if either HCQ or IVM stopped the COVID-19 infections early.
Why would Dr. Fauci care to undermine any medicine that might compete with remdesivir? Might it have something to do with NIAID and CDC having just spent $79 million developing remdesivir for Gilead, a company in which the Bill & Melinda Gates Foundation owns a $6.5 million stake? The BMGF is engaged in other large drug development deals with the company, including a co-funded $55 million investment in a malaria treatment being developed by Lyndra Therapeutics. Gates has also funded the promotion of Gilead’s Truvada in Kenya. Another Gilead partner, the US Army Medical Research Institute of Infectious Diseases at Ft. Detrick, Maryland (USAMRIID), where the drug was studied in monkeys, also contributed millions to remdesivir’s development. At the outset of the coronavirus plague, remdesivir was just another pharma-owned molecule that FDA had never approved as safe and efficacious for any purpose. In 2016, remdesivir demonstrated middling antiviral properties against Zika, but the disease disappeared before the expensive non-remedy got traction. After the Zika threat vanished, NIAID put some $6.9 million into identifying a new pandemic against which to deploy remdesivir. In 2018, Gilead entered remdesivir in a NIAID-funded clinical trial against Ebola in Africa.
This is how we know that Anthony Fauci was well aware of remdesivir’s toxicity when he orchestrated its approval for COVID patients. NIAID sponsored that project. Dr. Fauci had another NIAID-incubated drug, ZMapp, in the same clinical trial, testing efficacy against Ebola alongside two experimental monoclonal antibody drugs. Researchers planned to administer all four drugs to Ebola patients across Africa over a period of four to eight months.
However, six months into the Ebola study, the trial’s Safety Review Board suddenly pulled both remdesivir and ZMapp from the trial. Remdesivir, it turned out, was hideously dangerous. Within 28 days, subjects taking remdesivir had lethal side effects including multiple organ failure, acute kidney failure, septic shock, and hypotension, and 54 percent of the remdesivir group died—the highest mortality rate among the four experimental drugs. Anthony Fauci’s drug, ZMapp, ran up the second-highest body count at 44 percent. NIAID was the primary funder of this study, and its researchers published the bad news about remdesivir in the New England Journal of Medicine in December 2019. By then, COVID-19 was already circulating in Wuhan. But two months later, on February 25, 2020, Dr. Fauci announced, with great fanfare, that he was enrolling hospitalized COVID patients in a clinical trial to study remdesivir’s efficacy. For important context, this was a month before the WHO declared the new pandemic, a time that there were only fourteen confirmed COVID cases in the United States, most from the Diamond Princess cruise ship. These individuals were among the first wave of COVID-19 hospitalizations from whom NIAID recruited the 400 US volunteers for Dr. Fauci’s remdesivir trial. Dr. Fauci’s press release said only that remdesivir “has shown promise in animal models for treating Middle East Respiratory Syndrome (MERS).” It’s unclear, then, if NIAID informed these frightened souls that, less than a year earlier, a safety review board had deemed remdesivir unacceptably toxic.
Its deadly effect on patients aside, remdesivir was a perfect strategic option for Dr. Fauci. Optics required that NIH devote some resources to antiviral therapeutic drugs; critics would complain if he spent billions on vaccines and nothing on therapeutics. However, any licensed, repurposed antiviral that was effective against COVID for prevention or early treatment (like IVM or HCQ) could kill his entire vaccine program because FDA wouldn’t be able to grant his jabs Emergency Use Authorization. Remdesivir, however, was an IV remedy, appropriate only for use on hospitalized patients in the late stages of illness. It would therefore not compete with vaccines, allowing Dr. Fauci to support it without compromising his core business. Furthermore, while HCQ and IVM were off-patent and available generically, remdesivir was in the sweet spot of still being on patent. The potential profit upside was impressive. Remdesivir cost Gilead $10 per dose to manufacture. But by granting Gilead an EUA, regulators could force private insurers, Medicare, and Medicaid to fork over around $3,120.00 per treatment—hundreds of times the cost of the drug. Gilead predicted remdesivir would bring in $3.5 billion in 2020 alone.
Dr. Fauci did not suddenly get the idea that remdesivir might work against coronavirus in January 2020. In one of his many extraordinary feats of uncanny foresight, beginning in 2017, Dr. Fauci paid $6 million to his gain-of-function guru, Ralph Baric—a University of North Carolina microbiologist—to accelerate remdesivir as a coronavirus remedy at China’s biosecurity laboratory in Wuhan. Baric used coronavirus cultures obtained from bat caves by Chinese virologists working with Peter Daszak’s EcoHealth Alliance, another recipient of Dr. Fauci’s funding. Dr. Fauci demonstrated his personal interest in those experiments by dispatching his most trusted deputies, Hugh Auchincloss in 2018 and then Cliff Lane in 2020, to negotiate with the Chinese government and to supervise Baric’s experiments at the Wuhan lab and elsewhere in China. Baric claimed that his mouse studies showed remdesivir impeded SARS replication, suggesting that it might inhibit other coronaviruses. Chinese researchers at the Wuhan Lab and China’s Military Medicine Institute of the People’s Liberation Army Academy of Military Science submitted their own patent application for remdesivir. China’s military brass said the joint patent application was “aimed at protecting China’s national interests.”
Early in March 2020, the Gates Foundation bankrolled $125 million of tax-deductible grants to support drug makers to develop coronavirus treatments. Gates and/or his foundation had large equity stakes in many of the pharmaceutical companies that received these funds—including Gilead. On April 24, 2020, Gilead’s volunteer spokesperson Bill Gates declared: “For the novel coronavirus, the leading drug candidate in this category is remdesivir from Gilead.”
For HCQ, Dr. Fauci demanded well-designed randomized double-blind placebo-controlled trials and he warned against the use of IVM for treatment. In contrast, Fauci green- lighted remdesivir following studies in which the control group did not receive a real placebo. Instead, Fauci’s researchers used no placebo in the more severely ailing patients and gave the remaining patients an “active comparator” containing the same treatment protocol agents as used in the remdesivir arm except for substituting sulfobutyl for remdesivir as the test agent. Utilization of so-called “toxic” or “spiked” placebos— also known as “fauxcebos”—is a fraudulent gimmick that Dr. Fauci and his drug researchers have pioneered over forty years to conceal adverse side effects of toxic drugs for which they seek approval. Dr. Fauci eventually recruited 400 US hospitalized volunteers for NIAID’s remdesivir trials, but despite this fauxcebo chicanery, Dr. Fauci’s researchers just couldn’t get remdesivir to show any improvement in COVID survival.
Despite its disappointing performance, Dr. Fauci worked hand-in-hand with Gilead’s remdesivir team to guide the trial to a satisfactory outcome. According to Vera Sharav, the President and founder of the Alliance for Human Research Protection (AHRP), “The National Institute of Allergy and Infectious Diseases (NIAID) had complete control over the trial and made all decisions regarding trial design and implementation. Gilead Sciences employees participated in discussions about protocol development and in weekly protocol team calls with NIAID.”
Sharav’s organization, Alliance for Human Research Protection (AHRP), monitors the quality and ethical performance of clinical trials. NIAID’s remdesivir trial’s original endpoint made sense: to win approval, the drug would need to demonstrate a “reduction in COVID mortality.” However, the drug didn’t show the hoped-for benefit. While fewer patients receiving remdesivir died, those receiving remdesivir were also a lot less sick than the placebo subjects when they entered the trial. So Dr. Fauci’s team decided to move the goalposts. The researchers, in fact, had changed the trial “endpoints” twice in an effort to create a meager appearance of benefit. Dr. Fauci’s new endpoints allowed the drug to demonstrate a benefit, not by improving the chances of surviving COVID, but by achieving shorter hospital stays. Yet this too was a scam, because it turned out that almost twice as many remdesivir subjects as placebo subjects had to be readmitted to the hospital after discharge—suggesting that Fauci’s improved time to recovery was due, at least in part, to discharging remdesivir patients prematurely. Altering protocols in the middle of an ongoing study is an interference commonly known as “scientific fraud” or “falsification.” UCLA Epidemiology Professor Sander Greenland explains, “You’re not supposed to change your endpoint mid-course. That’s frowned upon.” Vera Sharav agrees: “Changing primary outcomes after a study has commenced is considered dubious and suspicious.”
But Dr. Fauci had little reason to worry that insiders would complain about the corruption of the study, since his trusted deputy, Cliff Lane, chaired the NIH Treatment Guidelines panel. Lane was doubly conflicted, since he had personally overseen the remdesivir trials in China, and stood, potentially, to share in patent rewards and royalties for the drug. In addition to Lane, seven of the panel members had financial relationships with Gilead—and eight additional panel members had had financial relationships with Gilead prior to the past eleven months, for which they were required to declare a relationship. “Is it any wonder remdesivir is the only drug recommended for COVID?” asks Vera Sharav, a Holocaust survivor who has devoted her life to advocating for ethics in the notoriously corrupt clinical trial industry.
Before his study was completed or peer-reviewed, much less published, Dr. Fauci learned that The Lancet had just published a placebo-controlled Chinese study that showed remdesivir utterly ineffective at keeping hospitalized patients alive OR reducing the duration of hospitalizations. Even more importantly, remdesivir did not reduce the presence of the virus in the blood. Worst of all, the Chinese study confirmed remdesivir’s deadly toxicity. The Chinese regulators and researchers shuttered that trial because of potentially lethal side effects. Remdesivir caused serious injuries in 12 percent of the patients, compared to 5 percent of patients in the placebo group. Unlike Dr. Fauci’s trial, the Chinese study was a randomized, double-blind, placebo-controlled, multi-center, peer-reviewed study, published in the world’s premier scientific journal, The Lancet. All the underlying data was available to the incurious press and the uninformed public.
In contrast, Dr. Fauci’s NIAID-Gilead study was at that point, still unpublished, not peer-reviewed, its details undisclosed. It employed a phony placebo and had suffered a sketchy mid-course protocol change. In April, the Chinese cancelled two ongoing clinical trials with NIAID in China because the Chinese had succeeded in ending the COVID epidemic in the country, and researchers could no longer identify enough COVID patients to enroll in the study.
In any event, the Chinese study spelled certain doom for remdesivir. It was now D.O.A. at FDA—a poem title? But Dr. Fauci never accepted this. The inimitable maestro of regulatory combat responded to the crisis with savvy and bold action that would miraculously salvage his sinking product: He appeared at one of his regular White House press conferences, this one in the Oval Office. Seated on the couch next to Deborah Birx and opposite President Trump, Dr. Fauci made a surprise announcement.
From that lofty platform, Dr. Fauci, with great fanfare, declared victory. The data from NIAID’s clinical trial for remdesivir shows “quite good news,” he said, glossing over the drug’s failure to demonstrate any mortality advantage. He boasted that the median time for hospitalization was eleven days for patients taking remdesivir, compared to fifteen days in the placebo group. He told the credulous press: “The data shows that remdesivir has a clear-cut, significant, positive effect in diminishing the time to recovery.” He claimed that his study had therefore proven remdesivir so remarkably beneficial to COVID patients that he had decided that it would be unethical to deny Americans benefits of this wonder drug. He was, he declared, unblinding and ending the study and giving remdesivir to the placebo group. Remdesivir would be America’s new “standard of care” for COVID. It was, of course, all a lie.
On May 1, the FDA granted the pandemic’s first Emergency Use Authorization for a COVID drug, allowing remdesivir treatments for patients hospitalized with severe COVID-19.
Based on Dr. Fauci’s representation, President Trump purchased the world’s entire stock of remdesivir for Americans. The European Union signed a “joint procurement agreement” with Gilead to queue up in the pipeline for 500,000 treatment courses. The day after Dr. Fauci’s announcement at the White House, the University of North Carolina issued a press release headlined: “Remdesivir, developed through a UNC-Chapel Hill partnership, proves effective against COVID-19 in NIAID human clinical trials.” Dr. Fauci’s gain-of- function wizard, Dr. Ralph Baric, called this “a game changer for the treatment of patients with COVID-19.”
Vera Sharav points out that in a rational universe, a poison like remdesivir would have no hope of winning regulatory approval—unless, of course, the company could somehow distract attention from the overwhelmingly catastrophic scientific evidence by getting the world’s most powerful health official—the man who conducted the clinical trial—to pronounce the drug a “miracle cure” at a globally attended press conference while lounging on an Oval Office divan beside the president of the United States. Says Sharav, “What better free advertisement?”
Sharav adds, “Dr. Fauci had a vested interest in remdesivir. He sponsored the clinical trial whose detailed results were not subject to the peer review he demanded for the drugs he regarded as rivals, like hydroxychloroquine and ivermectin. Instead of showing transparent data and convincing results, he did ‘science’ by fiat. He simply declared the disappointing results to be ‘highly significant,’ and pronounced remdesivir to be the new ‘standard of care.’ Fauci made the promotional pronouncement while sitting on a couch in the White House, without providing a detailed news release, without a briefing at a medical meeting, or peer review for publication in a scientific journal—as is the norm and practice, to allow scientists and researchers to review the data.”
“Standard of Care”
FDA’s recognition of remdesivir as the new “Standard of Care” for COVID meant that Medicaid and insurance companies could not legally deny it to patients and would have to fork over Gilead’s exorbitant price tag on a product US taxpayers had, by then, spent at least $85 million to develop. Improving Gilead’s business even more, doctors and hospitals that failed to use remdesivir could now be sued for malpractice, leading some medical experts to believe that coercing the use of this worthless and dangerous drug on COVID patients almost certainly cost tens of thousands of Americans their lives.
As we shall see, Dr. Fauci copied the choreographed script for winning remdesivir’s EUA from the worn rabbit-eared playbook that he developed during his early AIDS years, and then used repeatedly across his career to win approvals for deadly and ineffective drugs. Time and again, he has terminated clinical trials of his sweetheart drugs the moment they begin to reveal cataclysmic toxicity. He makes the absurd claim that his drug-du-jour had proven so miraculously effective that it would be unethical to deny it to the public, and then he strong-arms FDA to grant his approvals. This time only, the brazenness of the fraud earned Dr. Fauci some rare criticism even in mainstream science and press, and from academic institutions that customarily maintain silence about his shenanigans, given their addictions to whopping NIH and BMGF funding.
On October 24, 2020, Umair Irfan noted that “The FDA is once again promoting a Covid-19 therapy based on shaky evidence.”
The British Medical Journal pointed out, “None of the randomized controlled trials published so far, however, have shown that remdesivir saves significantly more lives than standard medical care.”
Eric Topol of Scripps Research Translational Institute scolded that, “This is a very, very bad look for the FDA, and the dealings between Gilead and EU make it another layer of badness.”
Angela Rasmussen, a virologist at Columbia University Mailman School of Public Health, told a reporter: “I was really surprised when I saw that news.”
Science Magazine said Dr. Fauci’s move had, “baffled scientists who have closely watched the clinical trials of remdesivir unfold over the past 6 months—and who have many questions about remdesivir’s worth.”
University of Oxford Professor of Clinical Therapeutics Duncan Richard scathingly observed that, “Research based on this kind of use should be treated with extreme caution because there is no control group or randomization, which are some of the hallmarks of good practice in clinical trials.”
Professor Stephen Evans in Pharmacoepidemiology, at the Gates-funded London School of Hygiene & Tropical Medicine, offered a particularly scathing assessment—“The data from this paper are almost uninterpretable. It is very surprising, perhaps even unethical, that the New England Journal of Medicine has published it. It would be more appropriate to publish the data on the website of the pharmaceutical company that has sponsored and written up the study. At least Gilead has been clear that this has not been done in the way that a high-quality scientific paper would be written.”
Even Bill Gates raised an eyebrow about the audacity of the caper. When Wired magazine in August 2020 asked Gates what therapeutic treatment he’d ask for if hospitalized with COVID- 19, he did not hesitate. “Remdesivir,” Gates replied, adding a comment that put daylight between him and the embarrassing clinical trial fiasco. “Sadly the trials in the US have been so chaotic that the actual proven effect is kind of small. Potentially the effect is much larger than that. It’s insane how confused the trials here in the US have been.”
* * *
Then, on October 19, 2020, three days before remdesivir’s FDA approval, the World Health Organization published a definitive study on remdesivir involving 11,266 COVID-19 patients in 405 hospitals and 30 countries. The power of this study dwarfed the Fauci/Gilead project, which had recruited 1,062 patients. In the WHO’s trial, remdesivir failed to reduce mortality, and failed to reduce the need for ventilators OR the length of hospital stays. WHO researchers found no detectable benefits from remdesivir and recommended against its use in COVID-19 patients. WHO published its devastating indictment of remdesivir one month after FDA issued the remdesivir EUA for children less than 12 years of age. Dr. Fauci and the FDA knew about the WHO study before the FDA issued the EUA for remdesivir, and almost certainly read the preprints and understood the findings. It appears, in fact, that Dr. Fauci once again hurried the approval through FDA so as to beat the publication of a negative study.
On July 15, 2021, a large Johns Hopkins Study in Original Investigation | Infectious Diseases once again confirmed that “Remdesivir treatment was not associated with improved survival but was associated with longer hospital stays.” (Emphasis added.)
On October 2, 2020, the European Union released its own safety review of remdesivir. The study reported serious side effects.
“Every independent randomized controlled trial of remdesivir has shown either a lack of benefit or a clear trend to harm,” says Dr. Pierre Kory. “It’s only those two Pharma studies (with Dr. Fauci) that show any benefits and even then, the benefits are minor.”
“It makes no sense to give an antiviral in late stages of a viral infection,” Dr. Kory adds. “The viral replication mainly takes place prior to day seven. If an antiviral works, that’s when you administer antivirals. Remdesivir might work early on, but we don’t know, because it’s IV administered and you can’t really do that to ambulatory patients.”
A Remedy Worse than the Malady
From early in May 2020, doctors and hospitals began using remdesivir on hospitalized patients who tested positive for COVID in PCR tests. By November 9, 2021, the publication date of this book, CDC’s website lists only two drugs approved for treating COVID-19, remdesivir and the corticosteroid dexamethasone. Doctors often use the two drugs in conjunction. Assessing remdesivir’s impact on hospitalized COVID-19 patients is difficult, in part, because—like COVID- 19—remdesivir causes extreme toxicity to lungs and kidneys, and mimics several of the other lethal symptoms of COVID, including multi-organ failure. Many doctors believe our country’s record COVID-19 fatalities are at least in part due to widespread use of remdesivir in 2020. “We had the most deaths worldwide,” says Dr. Ryan Cole. “It’s a haunting question: How many of these Americans were remdesivir casualties?”
For several months, we were the only country treating people with a drug proven to be lethal. That year, 2020, we had almost double the number of deaths per month compared to most other countries. Brazil, one of the first nations to widely use remdesivir, had the second highest death toll.
In May of 2020, New York doctors repeatedly marvelled at the tendency for COVID-19 to cause kidney failure, something that no other respiratory virus does. Doctors began seeing acute kidney failure on day three, four, and five after admission.82 Hospitals short on ventilators also ran out of dialysis machines. Physician and laboratory CEO Dr. Ryan Cole is one of many doctors who believe that many of those cases were attributable to remdesivir. “COVID-19 can affect the kidneys,” he says. “We know this because we can recover the spike protein from urine. But it’s dubious that the sheer magnitude of acute renal failure we saw among hospitalized COVID patients can all be attributed solely to the coronavirus infection.”
Dr. Cole told me that in the animal studies, one-fourth of the animals died from kidney failure. He explains that kidney collapse can lead to fluid accumulations in the lungs and everywhere and results in multi organ failure and sepsis—all of which are also sequelae of COVID. “Remdesivir shouldn’t be on the market,” he added.
Dr. Fauci’s 2019 Ebola study proved that remdesivir, by day three, four, and five, caused acute kidney failure in upwards of 31 percent of patients. In less than five days of remdesivir treatment, 8 percent of all people died or experienced life- threatening multiple organ failure or kidney failure so severe they had to be taken off the drug. “So it may not be a coincidence that roughly the same number of hospitalized COVID patients—8–10x were dying in the first week,” says Cole.
Dr. McCullough gives us a stark and clear summary: “Remdesivir has two problems. First, it doesn’t work. Second, it is toxic and it kills people.”
I am always looking for good, personal GMC, covid and childhood vaccination stories. You can write to me privately: unbekoming@outlook.com
If you are Covid vaccine injured, consider the FLCCC Post-Vaccine Treatment
If you want to understand and “see” what baseline human health looks like, watch (and share) this 21 minutes
If you want to help someone, give them a book. Official Stories by Liam Scheff. Point them to a safe chapter (here and here), and they will find their way to vaccination.
Here are all eBooks and Summaries produced so far:
FREE Summary: Bitten by Kris Newby (Lyme Disease)
FREE Summary: The Great Cholesterol Con by Dr Malcolm Kendrick
FREE Summary: Propaganda by Edward Bernays
FREE Summary: Toxic Legacy by Stephanie Seneff (Glyphosate)
FREE Summary: The Measles Book by CHD
FREE Summary: The Deep Hot Biosphere by Thomas Gold (Abiogenic Oil)
FREE Summary: The Peanut Allergy Epidemic by Heather Fraser
FREE eBook: A letter to my two adult kids - Vaccines and the free spike protein
What’s Really Ailing Us?
SUMMARY
Westerners are infested with pathogenic bugs such as molds, other fungi, intracellular parasites, etc.
Those infections come from many sources, including the ones that the doctors aren’t taught about. One of the sources is contaminated vaccines, not just COVID vaccines but also traditional vaccines (and it has been this way for decades).
In 2020, a number of stressors kicked those latent or near-latent infections into high gear.
Many classic COVID symptoms circa 2020 overlap with the symptoms of fungal pneumonia, bacterial pneumonia, pulmonary toxoplasmosis, etc. There are many bugs that can wreak havoc when the body is weak. I suspect we don’t even know all of them—and the diagnostic tools, from the patient’s perspective, mostly just effen suck.
Since the practical implications of my theory are much broader than “COVID,” and there is not even a consensus on what COVID is, I am going to focus on the things that matter gravely regardless of one’s position on the hot buttons, such as whether viruses exist, etc.
There are pathways from getting infected with one of those bugs to neurological issues, psychiatric issues, reproductive issues, blood clots, strokes, etc.
Personally, I believe that dementia and autism are infectious diseases with an incubation period that can last from a few days to decades. I believe that biological contamination is one of the big routes in which “vaccines cause autism,” with chemical and mechanical irregularities being a consequence rather than a primary cause of the disease. (On the other hand, injecting poisons sounds like a very inhumane idea.)
When they rolled out the COVID “vaccines,” those were far filthier than anything that had been rolled out before. The monstrosities were administered on a large scale to adults, and it “helped” the people to get new or additional “doses” of various bugs straight into their arms and their bloodstreams.
Both traditional and COVID vaccines have multiple issues, from contamination-related issues (magnetic beads and plasmids, anyone?) to platform-related issues, to toxin-related issues, etc. There is zero need to argue amongst ourselves and say, “No it’s not this, it’s that!” It’s probably this, and that, and many other things. For the sake of the suffering people, it’s good to examine all routes!
There seems to be is a strong correlation between the herbs and supplements that are thought to work against a number of fungi, parasites, etc., the herbs and supplements reported to work against COVID, and the herbs and supplements that, according to doctors treating vaccine injury, seem to help the people injured by COVID vaccines. Everyone is different, there certainly is no one-fits-all, and the journey may be long—but there is definitely a visible overlap.
My thinking is practical. I am not into arguing with people about fancy words. I have a strong gut feeling about this. If you find my theory of use to you, I am a happy … wait, damn you “new normal,” I can’t even say “happy camper” because it makes me think about isolation camps. Not a camper. A happy woman I am.
My request is to please test the damn vials. Please. Can you imagine how much easier it will be to talk to our mainstream friends and loved ones if they learned that “vaccine injury” can be explained by something as egregious as mold or pathogenic bacteria or parasites injected into their baby’s (or their parents’) arm?
The myth of cleanliness
We all know this script: We in the West are superior. We are clean. It is the dirty ones in the developing world who are infested with various dirty things of nature like fungi or parasites. Eeeeek. Not us!
Personally, I believe that the bodies of many westerners are populated with many unsexy bugs like molds, other fungi, intracellular parasites, etc. I believe that the reasons for this sad state of affairs are many but they are all very logical, not some cryptic rocket science. Both our microbiome and our environment are poisoned from here to horizon, and our immune systems are not what they used to be. At the same time, for decades now, people have been getting injected with diversely contaminated biologics, ushering a wide range of very lucky bugs straight into our arms--or straight into our bloodstreams--including the kinds of bugs that can grow slowly or sit out for long periods of time and make themselves very destructive only when an opportunity arrives (old age, a drop in immunity, extreme stress, etc.) At the same time, the scientists have been messing with synthetic biology, gene editing, and so on—and producing weird strains of organisms already known for their pathogenicity—as well as pathogenic artifacts the impact of whose interaction with human bodies is honestly unknown.
Come 2020, and…
Let us remember the premise of the theory: lots of westerners are walking around with unsexy latent infections that they have acquired in the course of their lives. Sometimes, they are walking around with them for years, undiagnosed. They are also walking with all sorts of other imbalances but for the sake of this story, let us focus on bugs.
They are walking around and walking around, maybe not too healthy but overall, feeling fine. And then—kaboom—something dramatic happens. Their bodies get bombarded with negative stimuli, their immunity drops—and that puts all latent infections and imbalances into high gear.
Now, in 2020, lots of things came into play. There was tremendous stress. There was an attack on social ties. There was an unprecedented increase in electromagnetic pollution due to Musk’s Starlink and the global 5G rollout. There was, possibly, a presence of synthetic biology particles known as SARS-CoV2. In addition to that, based on what my eyes saw, I believe there could also have been a massive hypnotic campaign that might have “animated” any hostile energy (such as bad bugs) that was already there.
Bottom line, whatever caused it, the infections that people had been previously walking with got kicked into high gear.
Now let’s look at the list of various COVID symptoms and see what other things can cause them
The lungs
I have written about it in the past, here is the link to the original article.
Let us ponder the COVID symptom that we’ve heard about a lot three years ago, “broken glass opacity” lungs. Here is a relatively sensible Insider article from March 13, 2020.
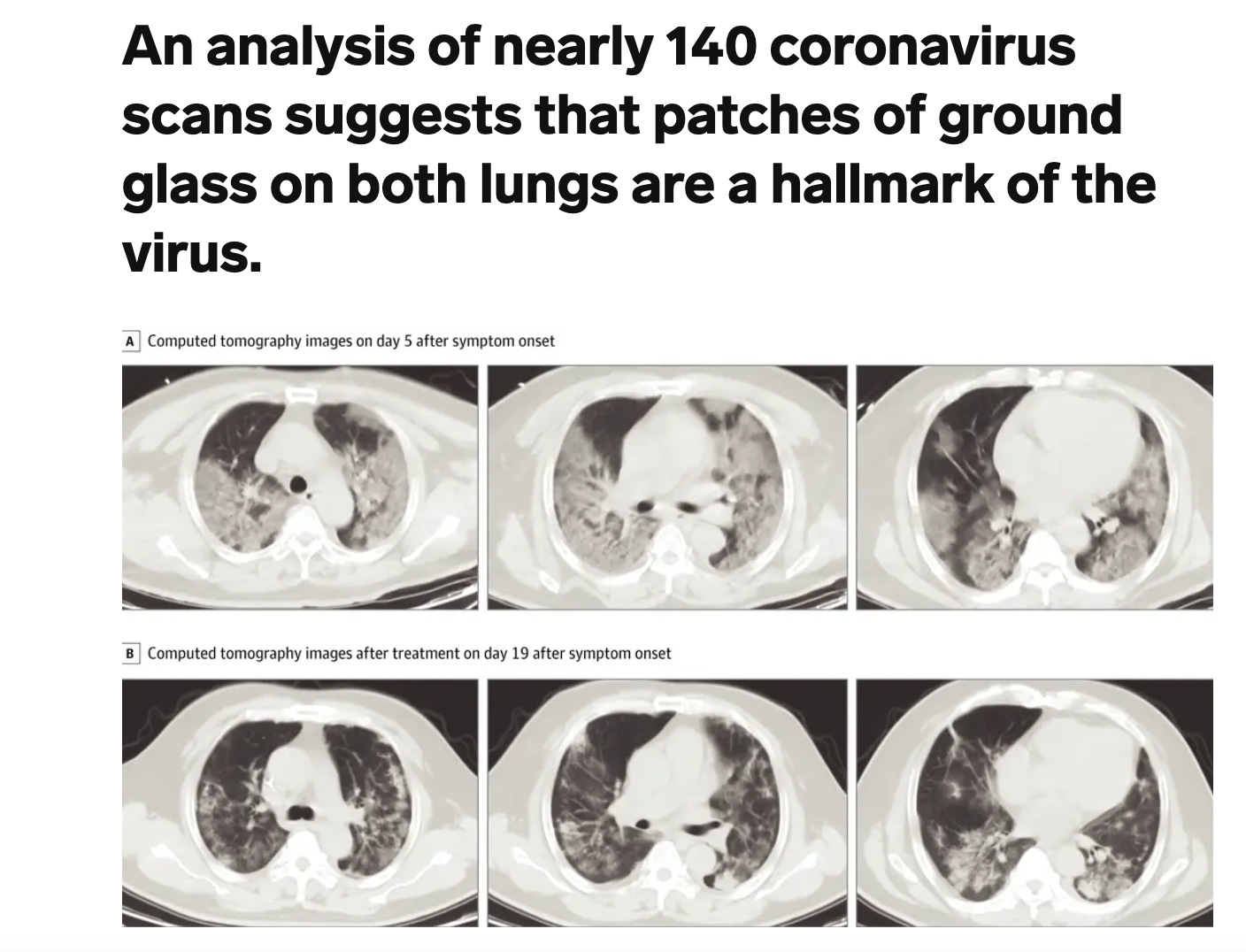
Of course, “broken glass opacity” lungs can result from many causes.
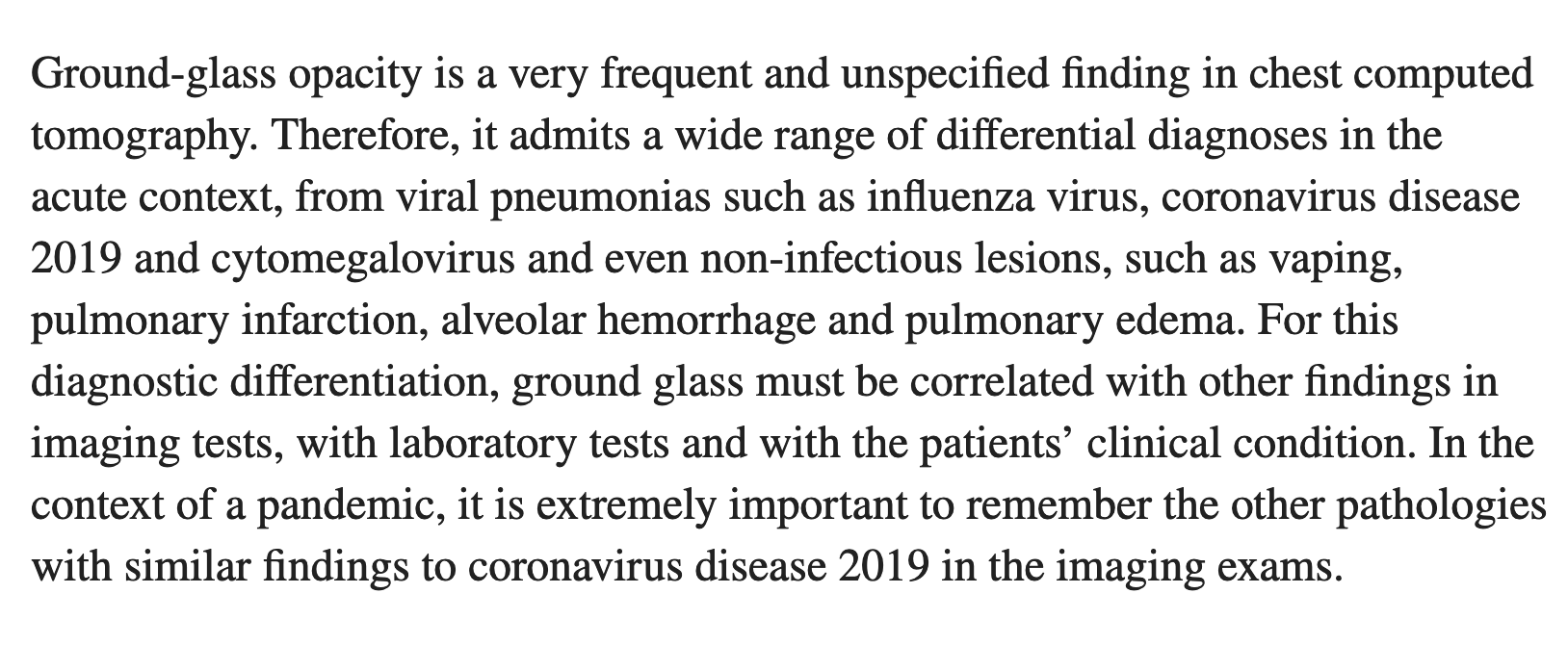
Here is one of the things that can is reported to cause it, hypersensitivity pneumonitis, also known as farmer’s lung. It’s a lung disease associated with exposure to organic dust.
To oversimplify, it can be triggered by exposure to mold. Is there a lack of mold? No. You can do an experiment and spray hydrogen peroxide on, say, the rubber part of the washing machine at the laundromat, and see it foam, which indicates that the surface is covered in live organic matter, most likely mold. On a side note, they say that mold can also grow in the lungs. And I bet you that until they come up with a lucrative injectable product to push on us, it is not going to be a “thing” to test for without the patient begging (and let’s pray that the injectable product they come up with is not contaminated with … mold, like those J&J vials).
See also “Mold infested air where Covid ‘vaccine’ ingredients are made for Moderna and Pfizer.”
What else can cause “broken glass opacity” in the lungs? One of the organisms that can cause it is toxoplasma, via pulmonary toxoplasmosis (also see the bolded text, please):
(I wrote about it earlier. It is very prevalent in the Western populations (theoretically estimated at 10-90% depending on the country). associated with dementia when they actually look, poorly diagnosed [in its cyst form] —and, great professional confidence notwithstanding, rather poorly understood.)
For the 51 pulmonary cases, the main clinical presentation was pneumonia or pleural effusions in 94% (48/51) and respiratory failure in 47% (24/51). For the 46 CNS cases, the main clinical presentation was encephalitis in 54% (25/46), meningitis in 13% (6/46), focal neurologic findings in 24% (11/46), cranial nerve palsies in 17% (8/46), Guillain–Barre syndrome or Miller Fisher syndrome in 7% (3/46), and Brown–Sequard syndrome in 2% (1/46) of cases; more than one clinical manifestation could also be present. Among the 41 CNS cases reporting the CNS imaging findings, 68% (28/41) had focal supratentorial lesions and 7% (3/41) had focal infratentorial lesions. Brain abscess-like/mass-like lesions were seen in 51% (21/41) of cases. For the 36 cardiac cases, the main clinical presentation was myocarditis in 75% (27/36), pericarditis in 50% (18/36), heart failure and/or cardiogenic shock in 19% (7/36), and cardiac arrhythmias in 22% (8/36); more than one manifestation could also be present. Illness was critical in 49% (44/90) of cases intensive care unit care was needed in 54% (29/54) of cases among those reporting this information, and 9 patients died. Conclusion: The diagnosis of severe toxoplasmosis in immunocompetent hosts can be challenging. [my point]
Toxoplasmosis should be considered in the differential diagnosis of immunocompetent patients presenting with severe illness of unclear etiology with pulmonary, cardiac, CNS, or multiorgan involvement/failure, or prolonged febrile illness, even in the absence of common exposure risk factors or common manifestations of toxoplasmosis (e.g., fever, mononucleosis-like illness, lymphadenopathy, and chorioretinitis). Fatal outcomes can also rarely occur in immunocompetent patients. Prompt initiation of anti-Toxoplasma treatment can be lifesaving.
And of course, bacterial pneumonia has been implicated in the pulmonary COVID symptoms even in the MSM. Also, it has been said many times that during the Spanish flu, it was bacterial pneumonia that the people were unfortunately passing from.
Here is what the NIH said:
Quite predictably, the NIH takes the usual route (“let us sell more vaccines, yo”). But at least they acknowledge bacterial pneumonia. And methinks, could it have been a whole range of pathogenic bugs, such as molds, bacterial, and parasites? I think it could have been.
Toxo clots?
Now let’s look more at toxo, a protozoan that is very prominently represented in the West, and how (I am hypothesizing) it can potentially create blood clots as a result of contaminated shots. I would like to emphasize that this is my theory based on thinking, logic, and reading, and I am not saying that there are no other factors at play. There are often many factors at play. It’s just that I am interested in this specific investigation, and I am writing about that.
Anyway, let us say, the vial is contaminated with toxo (very easy to imagine given the fact that, in the words of Sasha Latypova, those injections are “garbage soup.”) Let us say, the enthusiastic pharmacist administering the injection hits the blood. Well, this is a very vicious protozoan parasite, and it is capable of infecting endothelial cells. In fact, infecting endothelial cells is one of the ways it gets past the BBB and into the brain. But before it gets to the brain from that syringe, it can potentially infect the endothelial cells of the vessel they’ve been ushered in, which would lead to inflammation and, as a result of inflammation, clots. (I welcome input of all curious doctors, please).
Let us add additional factors (this is in a broader context than clots). Let us say that the injectee, in his or her prime, has a couple of latent infections going that are just sitting there in the back without causing much drama, waiting for their primetime. And then this thing goes into his blood, accompanied by toxic lipids, aspirational mRNA, and God know what else. And there is all this inflammation, and the immune system is stressed. That, now, would cause a cacophony of microbial wars where several sneaky pathogens could sense the opportunity and raise heads. And when microbial wars get complicated, so does the diagnosis—and given the cultural disconnect and the fact that the doctors rarely check for things like mold or toxo infections to begin with, and good diagnostics costs a lot, the fate of the patient depends on whether he is really lucky with the doctor, or whether he has the money to seek alternative diagnostics and treatments, etc.
Myocarditis
Quoting from the same article:
We’ve all heard a lot about myocarditis, and even the CDC says may be associated with the shots (“it’s rare,” blah blah blah)

The inflammation [of the heart muscle] can be triggered by many adversarial microbes, some of them we know, and some we probably don’t. That same protozoan, toxoplasma, can cause myocarditis, as do many other bugs.

Neurological problems, stroke-like symptoms, and Alzheimer’s Disease
There is a richness of literature showing links between various bugs inducing inflammation in the brain or CNS—and neurological problems such as seizures or sensory distortions, or stroke-like symptoms, or Alzheimer’s, or even psychiatric issues,, etc.
That alone deserves a series of articles. I wrote one for Dr. Mercola about the infectious theory of Alzheimer’s disease. Personally, I am subscribed to that theory and believe that the chemical or physiological changes that the researchers observe are in many cases the body’s reaction of the bugs. (But because our culture is very mechanistic, and the technical side is interesting and exciting to specialize in, the researchers focus on the technical side. Plus, to the best of my knowledge—and I asked and asked—diagnosing many of those bugs precisely can be tough. When researchers do animal studies, they kill the animals and look at their brains. It may be theoretically possible to diagnose human patients if the doctors were curious, open-minded, and able to pursue the correct diagnosis whatever it takes as far as costs—but I don’t think we live in that world.)
Until very recently, it was considered official and proven that Alzheimer’s Disease is non-infectious and caused by amyloid plaques
Last year, the news came out that the foundational study on Alzheimer’s that had been driving the overall direction of research in the past two decades had been based on fraud
The new emerging theory proposes that Alzheimer’s Disease may be triggered by pathogens, and amyloid plaques may form as an immune response
However, it is important to the remember that even if a pathogen or a group of pathogens is truly involved in triggering the symptoms of Alzheimer’s Disease, the mainstream narrative will be inevitably twisted in favor of pushing for more vaccines
Another article I wrote is about Toxoplasma gondii, who is a prime candidate for neurological disease.
At least one third of all people on Earth are infected with the parasite Toxoplasma gondii, averaging from 11-20% in the United States to 50% and higher in some Western European countries
The parasite has been implicated in ocular issues, schizophrenia, epilepsy, Alzheimer’s disease and various other neurological disorders, as well as in heart disease, pneumonia, recurrent headaches, even cancer; it is also known for causing psychological changes in its hosts
While the official word is that most toxoplasma infections are harmless and asymptomatic, the impact of the parasite could be much more devastating than the current mainstream medical convention presumes; it may also be cross-reacting with the spike protein and possibly contributing to the mystery of “long COVID”
According to recent research and clinical evidence, toxoplasma tissue cysts, previously considered harmless in immunocompetent patients, are capable of causing major health issues without converting to the cell-blasting form
Commonly used antibody tests can only detect antibodies for the “tachyzoite” (cell-blasting) form of the parasite but not the “bradyzoite” (tissue cyst) form
Dr Uwe Auf der Straße in Germany has done an important clinical investigation of the parasite, and his findings could shed light on “mystery” symptoms in many patients
Autism: the tragedy explained in different terms
Imagine a child. A baby. Let’s stay, that kid has one of those pathogenic but poorly diagnosed bugs, maybe from his mom, or maybe a clueless doctor injected him with an infectious vaccine. So now, this baby is tormented 24/7, there are microbes literally eating his brain, his head is abuzz, his brain is inflamed, he doesn’t feel good at all. So of course the kid is cranky and doesn’t want to socialize and does weird things to shake off the pain. What would you under the circumstance? Probably same thing. And of course he would have “learning disabilities,” he looks at things and to him, it’s as if there is a wall between him and whatever he is trying to understand, there is a wall, he can’t focus, and frankly, he doesn’t even have the energy to care due to perpetual head buzz.
And because he has been this way since an early age and has never felt discomfort-free enough to care about the outside world, he has never learned how to socialize or “read” others (he also doesn’t care to read anyone, he just wants the discomfort to end, but he doesn’t even know what it feels like to live without discomfort, he knows nothing “normal” to compare it to, all he knows about life is living with a perpetual torturous sensations in his head. Poor child!! Wouldn’t it be good to be actually able to help him? Yes, it would.
Once again, I believe that autism (as well as dementia) is to large extent an infectious disease. (As usual, life is complex, and there can be multiple factors, and yes, the pathogens do mess with various cellular functions, which is what the researchers often tend to look at without checking for living organisms triggering the change,, etc.)
Conclusion
All this tragedy is a logical consequence of the System of Domination and, I believe, a part of our philosophical journey from being poisoned to being healed. Now if only the good scientists and doctors got on this before the bad ones figure out how to spin it in order to sell us more poisonous vaccines….