
Decoding The Narrative
Decoding The Narrative
Pandemic, lockdown, vaccines, mandates, erosion of civil liberties, what does it all mean? Where does it lead? And how long before we get there? VOTING IN TWO WEEKS IN GENEVA...Write to your reps now!
Nearly half way through 2022 and we find ourselves still trapped in the Covid narrative with no real end in sight

This narrative is one part of an agenda that has many moving parts. You might be aware of some of them and you might be aware of some of the overarching goals. But how do we get from here to there? I’m going to attempt to decode the narrative based on what we’ve seen so far and what we know of certain globalist plans and layout a plausible timeline.
The often-maligned David Icke has a saying:
Know the outcome and you'll see the journey
This “outcome” is their plan for humanity. Who is this “they” I refer to? It’s the people that control this world. So, I hear you ask, who’s that? The Rockefellers? The Rothchilds? The central banks? The World Economic Forum? The CCP? The 13 Families of the Illuminati? (😂)
I don’t know about the Illuminati but all these actors play a role in furthering the overall agenda. They are all cogs in the complex machinery of the System. Whether there is an entity or entities at the helm of this System is the subject of much debate. Many people have theories, including myself, but we don’t need to get into the weeds of that debate because ultimately, we cannot know. What we do know is the architecture of the overt side of the System that governs humanity. Iain Davis of in-this-together.com and also a regular contributor to the excellent UK Column, calls the System “The Global Public-Private Partnership (GPPP)” and put together this chart to illustrate how policy is made, distributed, and enforced:
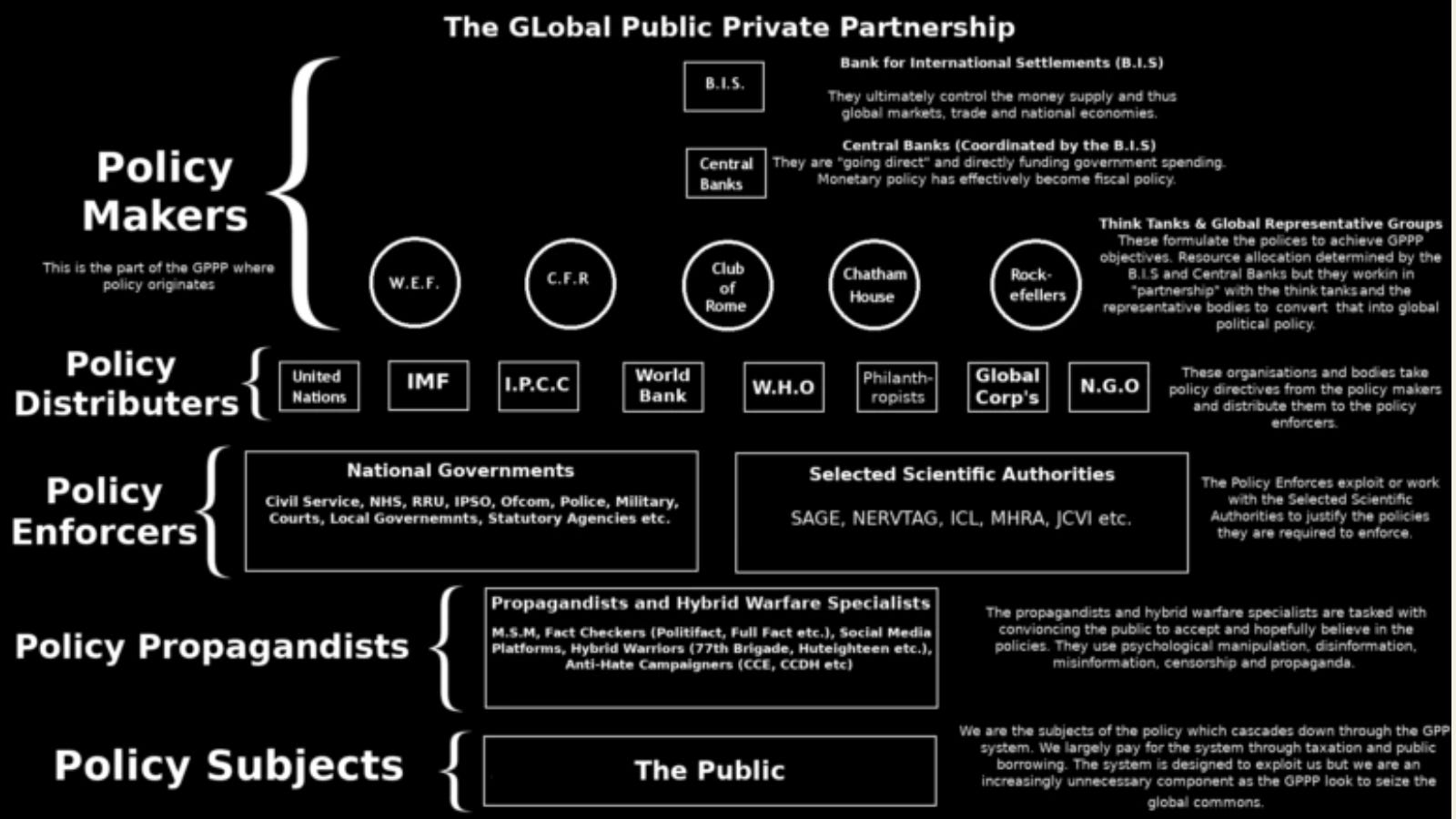
That’s a lot of Chiefs at the very top. It seems to me that in the Policy Makers we have 2 clear groups, central banks, and the globalist NGOs.
ON MAY 22: WHO WILL HAVE AUTHORITY TO LOCK DOWN ALL OF AMERICA
Officials from the Biden Administration are working to give the World Health Organization the power to unilaterally declare a health emergency in any country, thereby giving them emergency powers. The message from the administration and the vote are going unreported by the heritage media, but former Congressman Michele Bachmann is working hard at sounding the alarm.
BACHMANN: “BIGGEST GLOBAL POWER GRAB IN OUR LIFETIMES”
Bachmann has stated that the upcoming vote in Geneva over the Biden Administration’s amendments would cede U.S. sovereignty to the WHO over national healthcare decisions in what she described as “the biggest global power grab that we have seen in our lifetimes.”
It’s also interesting that Iain Davis lists “Rockefellers” alongside other Policy Makers such as WEF, CFR, and the Club Of Rome. However, let’s not forget that David Rockefeller founded the Council on Foreign Relations and the Club Of Rome. He was also a frequent attendee at Bilderburg Group meetings and the founder of the Trilateral Commission. Klaus Schwab, Executive Chairman of the World Economic Forum, was a student of Henry Kissenger’s at Harvard. Kissenger and David Rockefeller moved in the same circles and they were good friends. So we can infer some Rockefeller influence at the WEF too. Could it be that the Rockefellers control the geopolitical arm of the GPPP?
And if the Rockefellers have control over the geopolitical arm, what powerful family could possibly control global fiscal policy via the central banks? Who actually owns the Federal Reserve, the Bank Of England, and many others have been a hot subject in the conspiracy theory world. I’m not going to delve into that now, but if you’ve researched this topic you know who I’m talking about.
One thing missing from Iain’s diagram is the important role played by the asset management corporations such as Blackrock and Vanguard. It’s possible they have a seat at the Big Table too as they also seem to dictate economic policy. In 2019 it was a paper authored by Blackrock and discussed at the Jackson Hole conference that year, that outlined how the Fed would have to “go direct” when the next downturn hit. It did and they did. Blackrock and Vanguard manage assets to the tune of 16 trillion dollars, more than than the combined GDP of all 28 nations of the EU.
So we’ve established that “they” exist and if you want to read more about how the System works, please read Iain Davis’ excellent article.
So let’s move on to to the larger agenda. The first thing you need to realize is that everything you are seeing and experiencing is a smokescreen. For there is a problem, and it's a problem that seeks to undermine the very foundation of our society. Our financial system is about to implode. It is currently on life support, being kept alive by huge inflows of liquidity. This old system MUST be replaced, and soon, or the people that control this planet will lose it all.
The monetary system that is slated to replace the current one is Central Bank Digital Currency (CBDC). It would be wrong to compare this to cryptocurrency just because it sounds “digital”. And this is not digital money like we currently experience at our high street bank. With CBDC there is NO cash, it’s purely digital. This digital currency is issued direct from the central bank and there are no more high street banks. Your digital currency is accessed via a smartphone and without it, you can buy nothing. This gives the central bank complete control of your life. If they don’t like what you’re saying on social media, they can restrict your access to life. Didn’t get your 19th booster? Access denied. Your ability to interact with society can be deactivated at the flick of a switch. CBDC is digitally indentured servitude, free-range slavery.
If you think this sounds like a plot from a dystopian science fiction novel, I can assure you it is very real. All central banks are toying with their own version of CBDC right now. In the Bahamas, they are trialing it in real-time. Citizens have a CBDC account already. Some countries like Switzerland and Sweden have CBDC systems ready to go already. China’s digital yuan is rumored to be at a very advanced stage, spurring on the rest of the world to develop their own or face the consequences.
To learn more about CBDC is recommend the work of John Titus and his Best Evidence channel on YouTube.
So how does the current Pandemic narrative fit into the overall CBDC agenda?
CBDC is a digital control system. Due to the virus rampaging across the planet we now have these miraculous vaccines. To enforce vaccine uptake we now see the deployment of vaccine passports. The vaccine passport, green pass, health pass, whatever it’s called in your country is also a digital control system. The pandemic is a cover story for the introduction and normalization of a digital system that controls how you interact with society. It is a gateway to CBDC. Therefore we can expect to see widespread adoption of vaccine passports as this narrative continues to unfold. The UK just announced their Plan B which brings vaccine passports into existence. At first, it will be used for access to just a few venues, like nightclubs, but we can expect usage to widen in scope, slowly at first. We wouldn’t want the frogs to notice the water getting too hot, eh?
And if you’re in the US, thinking that with the legal challenges to vaccine mandates, the tide made me be turning, remember this was never about vaccines.

It also looks like Biden’s mandate, now reinstated by the 6th Circuit Court, is going to be decided by SCOTUS. This will be an enormous test and should it fail, it will spell impending doom. Even if the mandate is thrown out by SCOTUS corporate America will do the bidding of the System and slowly introduce and normalize the vaccine passport. The vaccine passport IS the instrument of our demise and we must fight it as if our lives depend on it, because they do.
In light of all this context, we can start to understand the insane push for mass vaccination when none of it makes any sense. How can you mandate a vaccine and exclude the elements of society that refuse when the vaccine doesn’t stop you from catching or transmitting it? Why is it that in the past, when a vaccine caused a few dozen deaths it would be withdrawn immediately, yet a vaccine that has caused more harm than ALL vaccines since records began is allowed to continue?
This was never about a virus. It was never about health. And it was never about vaccines. That should be starting to become clear now. They are necessary tools and they will be wielded like a cudgel in 2022.
Earlier this week I posted some predictions on Reddit and already the next phase in the narrative is being initiated. Lockdown Redux.

The UK is an excellent bellwether for this narrative. It’s a little less authoritarian and institutionally captured than its European counterparts but more so than the United States.
In spite of all reports that the new Omicron variant is extremely mild and no worse than the common cold, the UK government considered another lockdown.
The State Of CBDC
Lockdowns and mandatory vaccinations are looking to feature heavily in our immediate future. But what about CBDC?
In order to bring in this new system, the old system has to be destroyed. In spite of recent events, people are not that far gone that they will not recognize what the new system means for humanity. One can be very certain that a large proportion of people will not accept this form of disenfranchisement. It has to be dangled like a carrot, the solution to a problem so grave it will threaten to collapse civilization as we know it.
Problem, reaction, solution.
But what will be the nature of this "problem"? War - always a good candidate, right? No, too risky. You have to think about this through the lens of the people that want to bring about this change and that is financial. The destruction of the current financial system would bring everything to a stop and keep all the infrastructure intact. The collateral damage in human life would be enormous though. Famine, hunger, civil unrest, civil war, perhaps even local non-nuclear wars, all are on the table here.
From what I can deduce, the collapse mechanism all points to a major "cyberattack".

If you read the news I’m sure you’ll have heard chatter about a cyber attack. And as we know, once they start simulating things, they have a tendency to go live. A cyberattack on the global financial system would also nicely wipe out all the banks as they are no longer required anyway.
After a period of severe hardship, the system will be “fixed”. Society will return to normal, fuel will flow, supply chains will be restored. As no one has a job the global bank will also give you a stipend, a UBI, so you no longer have to eat your neighbors.
Along with the banks, any records of your asset ownership will be lost. So you'll need to surrender all assets to the state. Don't worry, because the state will now provide all you need. They will even give you a smartphone with your global digital ID that is connected to your central bank account.
Now you understand, “You will own nothing and you’ll be happy”.
You will love your servitude, slave, or else.
For an idea of timeline, you need to understand how quickly the CBDC technology is progressing. Also, we need to pay attention to the progress of vaccine passport adoption, the precursor to a global digital ID.
My current estimate is anywhere from 24-48 months. John Titus recently said he thinks CBDC is 3-4 years away. Political leaders have been repeating that they believe the war in Ukraine is going to go for another 3 years. If so, it’s been planned that way. But the system is vulnerable and unstable. It could crash by itself or it could be pulled anytime before then depending on how long they want to let society languish in limbo.
Pretty grim stuff. If you thought this was all about resisting vaccines, as bad as they are, the rabbit hole goes way deeper. People need to understand that we are at war, and we are not winning. And the stakes in this war could not be higher.
So what does one do?
We fight. We speak out. We protest. But ultimately this will be settled as all wars are. We need to prepare ourselves for that.

COVID Pills Cause Deadly Relapses and Supercharge Mutations
STORY AT-A-GLANCE
So far, all of the drugs developed against COVID-19 have been disastrous in one way or another. Remdesivir, which to this day is the primary COVID drug approved for use in U.S. hospitals, routinely causes severe organ damage and, often, death
Despite that, the U.S. Food and Drug Administration has approved remdesivir for in-hospital and outpatient use in children as young as 1 month old
Another COVID drug, Paxlovid, will in some cases cause the infection to rebound when the medication is withdrawn
Molnupiravir (sold under the brand name Lagevrio) also has serious safety concerns. Not only might it contribute to cancer and birth defects, it may also supercharge the rate at which the virus mutates inside the patient, resulting in newer and more resistant variants
The fact that U.S. health authorities have focused on these drugs to the exclusion of all others, including older drugs with high rates of effectiveness and superior safety profiles, sends a very disturbing message. They’ve basically become extensions of the drug industry, protecting the drug industry’s interests at the cost of public health
So far, all of the drugs developed against COVID-19 have been disastrous in one way or another. Remdesivir, for example, which to this day is the primary COVID drug approved for use in U.S. hospitals,1 routinely causes severe organ damage2,3,4,5 and, often, death.
Despite its horrible track record, the U.S. government actually pays hospitals a 20% upcharge for sticking to the remdesivir protocol, plus an additional bonus.6,7,8 Hospitals must also use remdesivir if they want liability protection.
Incentives like these have turned U.S. hospitals into veritable death traps, as more effective and far safer drugs are not allowed, and hospitals are essentially forced to follow the recommendations of the U.S. Centers for Disease Control and Prevention. As reported by Forbes science reporter JV Chamary back in January 2021, in an article titled, “The Strange Story of Remdesivir, a COVID Drug That Doesn’t Work”:9
“Remdesivir is an experimental drug developed by biotech company Gilead Sciences (under the brand name Veklury) in collaboration with the US Centers for Disease Control and Army Medical Research Institute of Infectious Diseases ...
The drug proved ineffective against the Ebola virus ... yet was still subsequently repurposed for SARS-CoV-2 coronavirus. News media prematurely reported that patients were responding to treatment.
But the published data10 later showed that ‘remdesivir was not associated with statistically significant clinical benefits [and] the numerical reduction in time to clinical improvement in those treated earlier requires confirmation in larger studies’ ...
What's weird about remdesivir is that it hasn't been held to the same standards as other drug candidates. Normally, a drug is only approved for use by a regulatory body like the U.S. Food and Drug Administration if it meets the two criteria for safety and efficacy.
Nonetheless, in October 2020, remdesivir was granted approval by FDA based on promising data from relatively small trials with about 1,000 participants. A large-scale analysis11 by the World Health Organization's Solidarity trial consortium has cleared-up the confusion.
Based on interim results from studying more than 5,000 participants, the international study concluded that remdesivir ‘had little or no effect on hospitalized patients with COVID-19, as indicated by overall mortality, initiation of ventilation, and duration of hospital stay.’ As a consequence of being mostly ineffective, WHO recommends against the use of remdesivir in COVID-19 patients.”
Shockingly, US Approves Remdesivir for Babies
Curiously, while Big Tech — aided and abetted by the U.S. government — has spent the last two years censoring and banning any information that doesn’t jibe with the opinions of the WHO, the U.S. government has completely ignored the WHO’s recommendation against remdesivir.
In fact, in late April 2022, the FDA approved remdesivir as the first and only COVID-19 treatment for children under 12, including babies as young as 28 days,12 which seems beyond Orwellian and crazy considering it’s the worst of both worlds: It’s ineffective AND has serious side effects.
What’s worse, the drug is also approved for outpatient use in children, which is a first. In an April 30, 2022, blog post,13 Dr. Meryl Nass expressed her concerns about the FDA’s approval of remdesivir for outpatient use in babies, stating:
“Remdesivir received an early EUA (May 1, 2020) and then a very early license (October 22, 2020) despite a paucity of evidence that it actually was helpful in the hospital setting. A variety of problems can arise secondary its use, including liver inflammation, renal insufficiency and renal failure14 ...
WHO recommended against the drug on November 20, 2020. Few if any other countries used it for COVID apart from the US. A large European trial15 in adults found no benefit. The investigators felt 3 deaths were due to remdesivir (0.7% of subjects who received it.) However, on April 22, 2022 the WHO recommended the drug for a new use: early outpatient therapy in patients at high risk of a poor COVID outcome.”
Remdesivir — A Reckless Choice for Children
Nass goes on to recount how monoclonal antibody treatment centers have been turned into outpatient treatment centers using remdesivir instead, but we still don’t have a lot of data on its effectiveness in early treatment. She continues:16
“The FDA just licensed Remdesivir for children as young as one month old. Both hospitalized children and outpatients may receive it. The drug might work in outpatients, but the vast majority of children have a very low risk of dying from COVID.
If 7 deaths per 1,000 result from the drug, as the European investigators thought in the study of adults cited above, it is possible it will harm or kill more children than it saves.
Shouldn’t the FDA have waited longer to see what early outpatient treatment did for older ages? Or studied a much larger group of children? Very little has been published on children and remdesivir ...
When we look at the press release17 issued by Gilead, we learn the approval was based on an open label, single arm trial in 53 children, 3 of whom died (6% of these children died); 72% had an adverse event, and 21% had a serious adverse event.”
Overall, remdesivir appears to be an exceptionally risky treatment choice for young children. Certainly, there are safer early treatment protocols that are very effective. Two other COVID drugs, Paxlovid and Molnupiravir, also have serious safety concerns.
Post-Paxlovid COVID Rebound
As reported by Bloomberg,18 COVID patients treated with a five-day course of Paxlovid sometimes experience severe rebound when the medication is withdrawn.19 U.S. government researchers are now planning to study the rate and extent to which the drug is causing SARS-CoV-2 infection to rebound, and whether a longer regimen might prevent it.
Bloomberg describes the post-Paxlovid rebound of David Ho, a virologist at the Aaron Diamond AIDS Research Center at Columbia University:20
“Ho said he came down with COVID on April 6 ... His doctor prescribed Paxlovid, and within days of taking it, his symptoms dissipated and tests turned negative. But 10 days after first getting sick, the symptoms returned and his tests turned positive for another two days.
Ho said he sequenced his own virus and found that both infections were from the same strain, confirming that the virus had not mutated and become resistant to Paxlovid. A second family member who also got sick around the same time also had post-Paxlovid rebound in symptoms and virus, Ho says.
‘It surprised the heck out of me,’ he said. ‘Up until that point I had not heard of such cases elsewhere.’ While the reasons for the rebound are still unclear, Ho theorizes that it may occur when a small proportion of virus-infected cells may remain viable and resume pumping out viral progeny once treatment stops.”
Clinical Director of the Division of Infectious Diseases at Brigham and Women’s Hospital, Dr. Paul Sax, told Bloomberg:21
“Providers who are going to be prescribing this should be aware that this phenomenon occurs, and if people have symptoms worsening after Paxlovid, it’s probably still COVID. The big problem is that when this drug was released, this information wasn’t included [on the label].”
Pfizer Defends Paxlovid
The U.S. Food and Drug Administration has stated it is “evaluating the reports of viral load rebound after completing Paxlovid treatment and will share recommendations if appropriate.” The U.S. Centers for Disease Control and Prevention has not yet commented on the findings.
Pfizer, meanwhile, insists the increase in viral load post-treatment “is unlikely to be related to Paxlovid” because viral rebound was found in “a small number” of both the treatment and placebo groups in Pfizer’s final-stage study.22 Clifford Lane, deputy director for clinical research at the National Institute of Allergy and Infectious Diseases (NIAID), told Bloomberg23 that some people may simply “need longer dosing of Pfizer’s drug than the standard five days.”
“There’s two things that suppress the virus: the drug and the host immune response,” he said. “If you stop the drug before the host immune response has had a chance to kick in, you may see the virus come back.”
Molnupiravir Supercharges Viral Mutation
Molnupiravir (sold under the brand name Lagevrio) also has serious safety concerns. This drug was developed by Merck and Ridgeback Therapeutics and approved for emergency use by the FDA December 23, 2021, for high-risk patients with mild to moderate COVID symptoms.
However, not only might it contribute to cancer and birth defects, it may also supercharge the rate at which the virus mutates inside the patient, resulting in newer and more resistant variants.24 As reported in November 2021 by Forbes contributor and former professor at Harvard Medical School, William Haseltine, Ph.D.:25
“... I believe the FDA needs to tread very carefully with molnupiravir, the antiviral currently before them for approval. My misgivings are founded on two key concerns.
The first is the drug’s potential mutagenicity, and the possibility that its use could lead to birth defects or cancerous tumors. The second is a danger that is far greater and potentially far deadlier: the drug’s potential to supercharge SARS-CoV-2 mutations and unleash a more virulent variant upon the world ...
My concern with molnupiravir is because of the mechanism26 by which this particular drug works. Molnupiravir works as an antiviral by tricking the virus into using the drug for replication, then inserting errors into the virus’ genetic code once replication is underway. When enough copying errors occur, the virus is essentially killed off, unable to replicate any further ...
But my biggest concern with this drug is ... molnupiravir’s ability to introduce mutations to the virus itself that are significant enough to change how the virus functions, but not so powerful as to stop it from replicating and becoming the next dominant variant.”
Haseltine cites prepandemic experiments showing MERS-CoV and the mouse hepatitis virus (MHV) both developed resistance against the drug, thanks to mutations that occurred. While the central idea behind the drug is that the genetic errors will eventually kill the virus, these experiments showed the viruses were in fact able to survive and replicate to high titers despite having large numbers of mutations throughout their genomes.
The drug did slow down replication, but as noted by Haseltine, “outside of the lab, as the drug is given to millions of people with active infections, this disadvantage may quickly disappear as we would likely provide a prime selection environment to improve the fitness of the virus.” This risk may be particularly high if you fail to take all the prescribed doses (typically 800 milligrams twice a day for five days).
Experts Question Usefulness of Molnupiravir
More recently, in a January 10, 2022, article, Newsweek cited concerns by professor Michael Lin of Stanford University:27
“’I am very concerned about the potential consequences now that molnupiravir has been approved ... It would only be a matter of time, perhaps a very short time, before a lucky set of mutations occurs to create a variant that is more transmissible or immunoevasive ...
The drug simply speeds up that natural process. The hope is that over enough days all the viral copies will have so many mutations that none of the copies can function.’ But Lin said he was concerned that in the real world, there is a possibility that a mutated virus could jump from a patient taking molnupiravir to another individual, citing the relatively modest efficacy of the drug.
‘For cases that get worse so that people have to go to the hospital, this drug only prevents that from happening 30%of the time. That means 70% of the time the virus isn't being eliminated quickly enough to make a difference. And we know COVID patients going to hospitals are highly contagious.’
Lin said the risks could be heightened when a patient does not comply exactly with the dosing schedule of the drug ... ‘In any of those situations viruses will have picked up some mutations but not enough to kill all the virus copies,’ he said. ‘The survivors are now mutated, perhaps have picked up immunoevasion, and can go on to infect others’ ...
According to Lin, the ‘very low efficacy alone’ should have disqualified the drug from approval ... ‘Even if the drug were great we wouldn't take such a risk, but this drug is worse than any other drug that's sought approval for COVID-19. It's completely not worth it.’”
Haseltine also told Newsweek28 that, “Of all the antiviral drugs I have ever seen, this is by far the most potentially dangerous,” and “The more people that take it, the more dangerous it will be.”
Even if the probability is very low, 1 in 10,000 or 100,000, that this drug would induce an escape mutant which the vaccines we have do not cover, that would be catastrophic for the whole world. ~ James Hildreth, president of Meharry Medical College
One of the FDA panel members who actually voted against the approval of molnupiravir, James Hildreth, president of Meharry Medical College in Tennessee, wanted Merck to do a better job of quantifying the risk of mutations before approval. During the panel meeting, he noted that:29
“Even if the probability is very low, 1 in 10,000 or 100,000, that this drug would induce an escape mutant which the vaccines we have do not cover, that would be catastrophic for the whole world.”
Government Has Sold Out to Big Pharma
Widespread use of a drug that turbocharges mutation of an already rapidly mutating virus probably isn’t the wisest strategy. Likewise, using drugs that cause high rates of organ failure, like remdesivir, and drugs that causes the virus to rebound with a vengeance, like Paxlovid, don’t seem to be in the best interest of public health either.
The fact that U.S. health authorities have focused on these drugs to the exclusion of all others, including older drugs with high rates of effectiveness and superior safety profiles, sends a very disturbing message.
They’ve basically become extensions of the drug industry and have abandoned their original purpose, which is to protect public health — by ensuring the safety and efficacy of drugs, in the case of the FDA,30 and by conducting critical science and data analysis in the case of the CDC.31
Instead, they seem to be doing everything they can to protect Big Pharma profits, even if it costs you your life. Remdesivir, for example, is an extremely expensive drug, costing between $2,340 and $3,120 depending on your insurance.32
Ivermectin, meanwhile — which has been very effective against COVID and shown to outperform at least 10 other drugs, including Paxlovid33 — costs between $4834 and $9435 for 20 pills depending on your location. The average cost is said to be about $58 per treatment.36
Paxlovid costs $529 per five-day course of treatment,37 and molnupiravir is around $700.38 While not quite as expensive as remdesivir, both are still nearly 10 times costlier than ivermectin, which is more effective. Paxlovid alone has cost U.S. taxpayers $5.29 billion. Just imagine the billions we could have saved had we saner leadership.
Since the FDA and CDC cannot be trusted, it’s imperative to take responsibility for your own health. Do your own research and follow your own conscience and conviction. Remember, when it comes to COVID-19, early treatment is crucial, and effective protocols are readily available — just not from the FDA, CDC or even most hospitals.
For a refresher, check out Dr. Pierre Kory’s interview with Chris Martenson.